Newborn Hearing Screening
 Alabama's Listening! is the Early Hearing Detection and Intervention Program (EHDI) for the Alabama Department of Public Health. The program was initiated in February 2001 to ensure all Alabama birthing facilities were able to screen for newborn hearing loss, which is the most commonly occurring birth disorder in the United States.
Alabama's Listening! is the Early Hearing Detection and Intervention Program (EHDI) for the Alabama Department of Public Health. The program was initiated in February 2001 to ensure all Alabama birthing facilities were able to screen for newborn hearing loss, which is the most commonly occurring birth disorder in the United States.
In 2008, Universal Newborn Hearing Screening (UNHS) became a mandated part of the Alabama Newborn Screening panel of disorders. The goal of the program is to create and maintain UNHS programs in Alabama to ensure early identification, treatment, and intervention of infants with hearing loss.
Newborn Hearing Reporting Forms
Alabama's Early Intervention System
Any child who has been identified with a hearing loss diagnosis should be referred for early intervention services as early as possible. Alabama's Early Intervention System is a coordinated, family-focused system of resources, supports and services for eligible infants and toddlers birth to 3 years who have developmental delays. Early Intervention services are defined by the federal Individuals with Disabilities Education Act (IDEA). Services may include:
- audiology
- assistive devices and technology
- occupational therapy
- physical therapy
- physchological services
- sign language and cued language speech services
- speech language pathology
- transportation
- vision services
To utilize Alabama's Early Intervention System, fax a completed referral form to (334) 293-7393.
Newborn Hearing Screening: What Do the Results Mean?
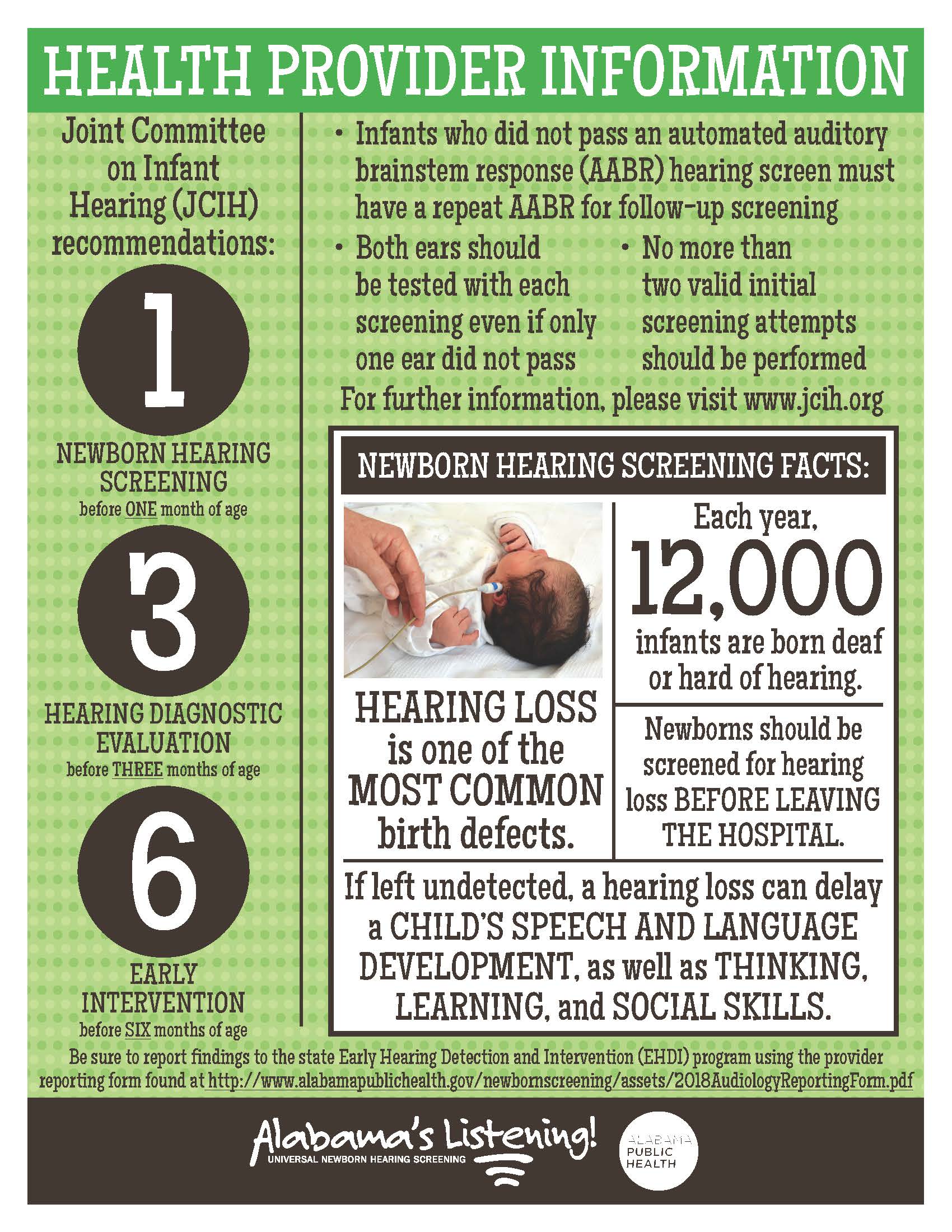
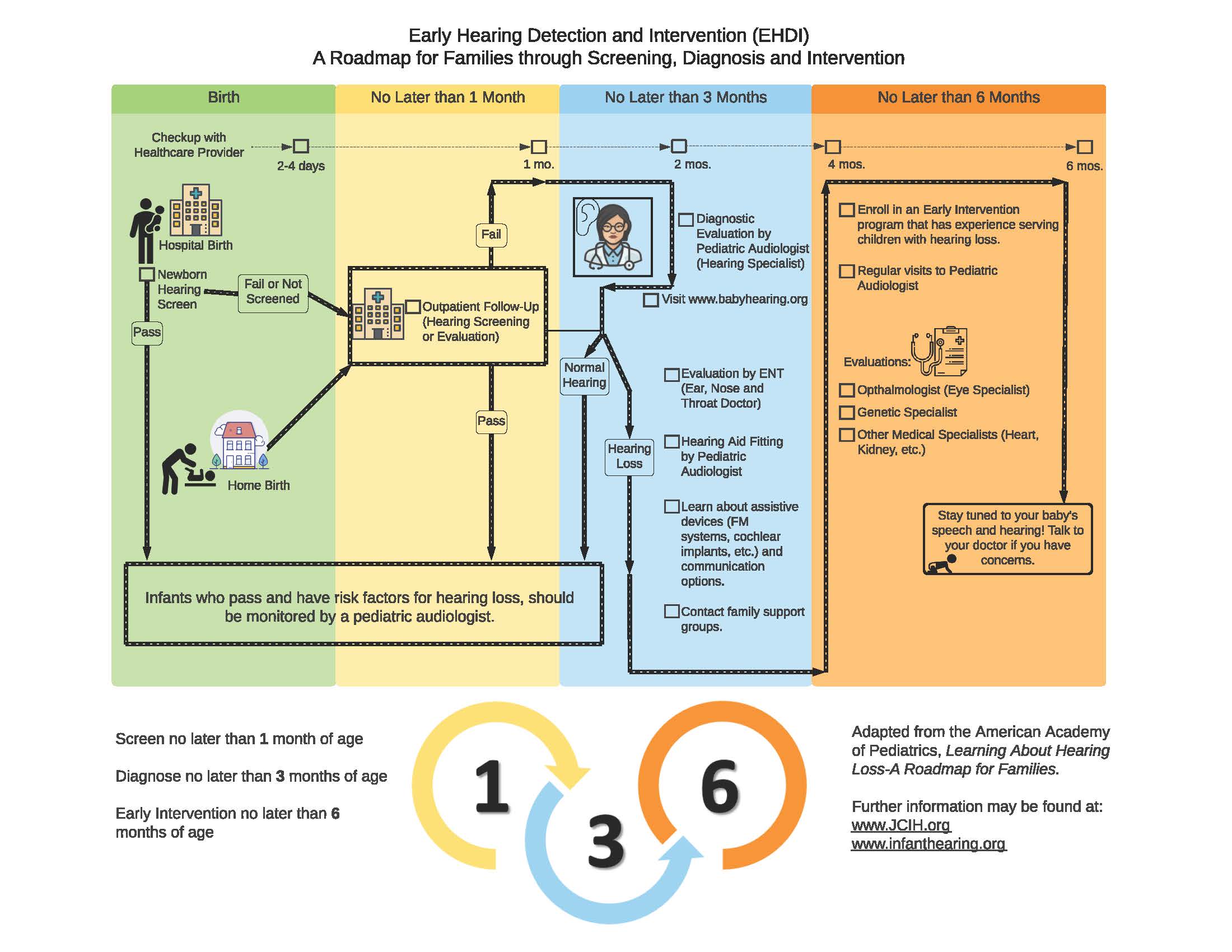
Hearing screening is performed at 24-48 hours of age, or before the baby leaves the hospital. Parents and health care providers can learn more about the process from our Newborn Hearing Screening flyer.

What if My Baby Passes the Newborn Hearing Screening but Has a Hearing Risk Factor?
According to the Joint Committee on Infant Hearing (JCIH), some infants who pass newborn hearing screening at birth may be identified later in childhood as deaf or hard of hearing. Hearing loss identified later in childhood is known as late onset or progressive hearing loss.
Some common risk factors for late onset hearing loss includes a hospital stay greater than 5 days and parent concern. The Hearing Risk Factor Card identifies risk factors which are known to be associated with late onset or progressive hearing loss. It is recommended a child receive another hearing evaluation by a pediatric audiologist between 3-9 months of age if a risk factor is identified. You may speak to your child's doctor at anytime if there is concern regarding your child's hearing development.
2021 Hospital Guidelines for Universal Newborn Hearing Screening
The Hospital Guidelines for Universal Newborn Hearing Screening provides guidance to hospitals on public health law, reporting requirements, training, screening tips, algorithms,scripts, risk factors, outsource considerations, and other information. Hospitals are encouraged to refer to the guidelines to be consistent with national standards.
Hospital Loaner Hearing Equipment
In case of equipment malfunction, notify the Alabama EHDI Program at 1-866-928-6755, and have a written protocol to ensure newborn hearing screening is performed prior to hospital discharge or by one month of age. If the infant is scheduled to have an outpatient hearing evaluation, results should be reported to the Alabama EHDI Program at fax (334) 206-3791. Please see the
Re-screen Newborn Hearing Results Form.
Alabama Early Hearing Detection & Intervention (EHDI) Workshop
The Alabama Department of Public Health Newborn Screening Program hosted the first EHDI Workshop on Friday, April 27, 2018, at the Alabama School for the Deaf and Blind (AIDB) in Talladega, Alabama. Thank you to all the presenters and participants for making the program a success. Thank you to AIDB for all of their assistance in planning the event and for use of their fabulous facilities.
Presentations included the following:
- Alabama EHDI Program Overview
- Hearing Equipment Demonstration
- Children's Rehabilitation Service Program Overview
- Early Intervention System Overview
Family Based Organizations
The Alabama Department of Public Health has partnered with Hands & Voices of Alabama, Guide By Your Side Program, to provide mentorship and support services to families who have a child identified with hearing loss. Services include regular support from parent mentors, training for various communication modes, and opportunities to collaborate with policy makers and the Early Hearing Detection and Intervention Program.
If interested in connecting with a parent mentor, please call Hands & Voices of Alabama Guide By Your Side Program at (205) 677-3136 or email [email protected].
Congenital Cytomegalovirus (CMV) and Hearing Loss
Congenital CMV is the most common non-genetic cause of childhood sensorineural hearing loss. According to the CDC, about one out of every 150 babies are born with congenital CMV infection. However, only about one in five babies with congenital CMV infection will be sick from the virus or will have long-term health problems such as hearing loss.
Some babies without signs of congenital CMV infection at birth may have hearing loss. Hearing loss may be present at birth or may develop later in babies who passed their newborn hearing test. Congenital CMV infection can be diagnosed by testing a newborn baby's saliva, urine, or blood. Such specimens must be collected for testing within two to three weeks after the baby is born in order to confirm a diagnosis of congenital CMV infection. For more information visit the CDC webpage.
 Online Resource: Hearing Service Directory
Online Resource: Hearing Service Directory
Early Hearing Detection & Intervention Pediatric Audiology Links to Services (EHDI-PALS) is a new easy-to-use online directory that helps families find the nearest clinic providing the type of hearing service their child needs. Visit EHDI-PALS for more information.
Newborn Hearing Podcast
The Earworm Podcast features conversations with a wide array of professionals, family members, advocates, and scientists whose experiences, ideas, curiosities, and activities are committed to ensuring that all children who are deaf or hard-of-hearing can thrive. The Earworm Podcast is available for streaming anywhere you listen to podcasts, as well at earwormpodcast.org.
Some of the Earworm podcasts are listed below:
- Episode 5: The Potential of Preventing the Most Common Non-Genetic Cause of Hearing Loss with a Vaccine/Interview with Dr. Lori Panther
- Episode 4: New Frontiers in Universal Hearing Screening: Genetic Screening/Interview with Dr. Eliot Shearer
- Episode 3: Diagnosing Why? The importance of knowing the cause of a child's hearing loss/with Dr. Eliot Shearer
- Episode 2: Newborn Screening Isn't Enough: A parent's perspective on late identified hearing loss/with Valerie Abbott
- Episode 1: Newborn Screening Isn't Enough: Monitoring Hearing Status Throughout Early Childhood/with Dr. Dylan Chan
Learn to Screen
Standardized online hearing screener training is available for pure tone audiometry courses and otoacoustic emissions courses through the National Center for Hearing Assessment and Management. The training is available for staff responsible for providing evidence-based hearing screening and follow-up services in Early Head Start, Early Intervention Programs, Preschool Programs, Home Visiting Programs, schools, and health care settings.
The training is intended for first-time screeners or for those previously trained who are needing a refresher. Once you complete the learning activities, you will obtain a personalized Certificate of Completion.
Online American Sign Language (ASL) Courses
Gallaudet University offers online ASL courses. Registrants can complete the courses at their own pace. Online courses are available year-round.
Reporting Requirements for Hearing Screening
Each year, the Centers for Disease Control and Prevention's (CDC) Early Hearing Detection and Intervention Program (EHDI) conducts the Hearing Screening and Follow-up Survey (HSFS). This survey is designed to collect national data on the number of infants screened, diagnosed, and referred to early intervention for hearing loss, in an effort to monitor the state's efforts in meeting the national EHDI goals. For a comprehensive view of the data provided to the CDC and to see how Alabama compares to other states, you can access the HSFS at the CDC website.
Newborn Hearing Screening Resources
- AAP EHDI Tip Sheet
- Akouos Resonate Family Brochure
- Akouos Resonate Family Brochure - Spanish
- Alabama Hands & Voices Training on Educational Advocacy
- Alabama Hands & Voices Advocacy Training - ASTRA
- Alabama Hearing Loss Options for Families
- American Sign Language Class - Register Online
- Association for the Deaf and Hard of Hearing: Parent and Infant Financial Aid Program
- Best Practice Letter- EHDI Program
- CDC Early Hearing Detection and Intervention Resources
- CDC Milestone Tracker App
- CMV Ends With Me Video Campaign
- CRS Hearing Clinics
- Early Hearing Detection and Intervention Checklist for Pediatric Medical Providers
- Free Genetic Testing for Parents
- Joint Committee on Infant Hearing (JCIH) Position Statement
- Learning Language in the Womb
- National Center for Hearing Assessment and Management (NCHAM) "It's Natural" Video
- NCHAM Newborn Hearing Screening Training Curriculum
- Newborn Hearing Screening Hospital Algorithm
- Open Provider Letter
- Opening the World of Sound: University of South Carolina Video of Hope
- Pathways for Famililes of Children Who are Deaf and Hard of Hearing
- Why Early Literacy Matters
- WISE Handout - NEW
- WISE Mobile Resource for Kids
- Wooley Institute for Spoken-Language Education (WISE) Early Intervention Program
- Wooley Institute for Spoken-Language Education (WISE) Family Nest
Developmental Milestones in Hearing
Parents can use this as a guide to see how their child is progressing developmentally.
Birth to three months:
- Jumps or blinks to loud sounds
- Wakes up to loud sounds
- Quiets when he or she hears mom's voice
Three months to six months:
- Turns eyes or head to search for the sound source
- Responds to your voice even when you cannot be seen
- Enjoys toys that make sounds
- Starts babbling
At six months:
- Responds to his or her name
- Turns head to the direction of the sound source
- Begins to imitate speech sounds
At 10 to 12 months:
- Understands and follows simple directions
- Gives a block or toy to you when asked for it without pointing
- Imitates speech sounds of others
At 13 to 18 months:
- Follows simple one step directions
- Uses 3-20 single words
- Points to 1-3 body parts when asked
At 19 to 24 months:
- Understands approximately 300 words
- Puts two words together ("eat cookie") by 24 months of age
- Points to five body parts
- Responds to "yes" or "no" questions
Every Baby Should Have a Hearing Screening
Statistics show that between 1 to 6 newborns per 1,000 have some degree of hearing loss. Although these statistics indicate that it is unlikely that most babies will have a hearing loss, it is important to identify existing loss as soon as possible since the first two years of a baby's life are critical for learning speech and language. Because any hearing loss could affect a baby's speech and language development, diagnosis and appropriate intervention should occur by 6 months of age or earlier.
Hearing Screening Methods
There are two types of hearing screens that may be used to test for hearing loss. Both tests are very safe, take only minutes to perform, and are non-invasive. Most infants sleep though the hearing screening procedure.
- Automated Auditory Brainstem Response (AABR): A soft click is presented to each ear through miniature earphones while electrodes placed on the infant’s forehead, neck, and shoulder record the response as it travels between the ear and brain. The response is analyzed to determine how well the inner ear and auditory nerve are working. This test method is recommended for high-risk newborns admitted to the NICU greater than five days and should be completed as a second test method if an infant is initially tested with AABR.
- Otoacoustic Emissions (OAE): Soft clicks or tones are presented into the infant’s ear through a probe snugly placed in the entrance to the ear canal. A small microphone in the probe measures the echo that returns from the infant’s ear. The OAE equipment analyzes this echo and determines how well the inner ear is working.
Hearing Screening Results
If an infant does not pass the first hearing screen, an attempt may be made to repeat the screen before hospital discharge, or it may be scheduled after going home. If an infant does not pass the second hearing screen, additional hearing tests should be administered under the care of an audiologist or otolaryngologist.
Although only a small percentage of infants who do not pass the hospital hearing screen actually have hearing loss, it is important for every baby to receive appropriate testing to adequately determine hearing ability. Also, because early intervention is so important to the development of infants with hearing loss, it is important that the testing not be delayed. It is recommended that all testing be completed by three months of age and that infants with hearing loss be enrolled in an intervention program as early as possible, but no later than six months of age. An audiologist and/or physician can provide information on local early intervention programs, or the information can be obtained by calling 1-800-CHILD-FIND (1-800-543-3098).
Retesting May Be Needed
The results of the a hearing test indicate an infant's hearing ability at the time of the test. Some children with recurrent ear infections, serious acute or chronic illness, or with a family history of hearing impairment , or other risk factors may develop hearing loss later in life. If there are ever any concerns about a child's hearing ability, or speech and language development, this should be addressed by the parents and the physician in order for an appropriate evaluation is to be completed.
Page last updated: December 12, 2025

